Interventions
The study design called for two interventions. The AMI was a face to face 30 minutes to one hour long intervention with participants, tailored to their intervention needs as determined by their scores below an established cutoff point on each of the study mediators. The Oral Health Fair / Campaign was a three session oral health fair, conducted in each building in collaboration with residents who formed a building based steering committee of people who were not eligible for participation in the project but wanted to contribute. The interventions are described in detail below.
Click here to view the frequently asked questions in both english and spanish
Adapted Motivational Interview
In preparation for a session, the interventionist custom-constructs a focal point checklists based on results from the participant’s baseline survey and clinical assessment. The clinical assessment shows the amount of plaque on a participant’s teeth. The survey provides information on 12 areas or ‘domains’ that focus on Activities for Daily Living (ADLs), incorrect beliefs, gaps in knowledge, gaps in self efficacy and limitations in intentions to practice and gaps in reported skills and specific oral hygiene practices. A computer program identifies where participants score below a predesignated cutoff point and transfers it to a standardized computer form that is used by the interventionist to guide the approach for each participant. A summary of this data outlining the participant’s cognitive and behavioral status pre-intervention is developed using standardized forms in english and spanish. The summary is used to conduct the intervention on areas where the participant scores fall below pre-established cutoff points on each of the 12 domains in the survey.
AMI-PM Session Outline
During each AMI-PM session, the interventionist:
- Re-confirms that the participant has agreed to have the session recorded for quality checking.
- Discusses with the participant the importance of taking care of teeth, mouth, gums in keeping one well and healthy, as well as any concerns that the participant may have regarding his/her own oral health.
- Explains that their just-completed survey identified areas the need attention to improve their oral health and shows the focal point worksheet which outlines these areas. Click here to view the focal point worksheet.
- Reviews each of the focal points (the domains scoring below the cutoff point on the survey results) on the checklist. The interventionist should probe for reasons that the participant has certain concerns, fears etc.
- Shows participant the plaque score results of his/her own clinical assessment. Click here to view an example of plaque score results.
- Shows videos demonstrating oral hygiene skills (brushing, flossing, cleaning dentures/partials).
- Demonstrates proper oral hygiene skills using mouth models. Click here to view oral hygiene skills demonstration.
- Asks participant to demonstrate how he/she brushes & floss (& cleans dentures if appropriate) using mouth model. The interventionist scores the participant’s brushing and flossing (and denture care if needed) ability as Excellent, Good, Fair, or Poor using criteria outlined in the “AMI-PM” Oral Hygiene Skills Assessment Evaluation Form
- Reviews concerns outlined in focal point checklist and works with participants to develop a cognitive behavioral plan to improve his/her oral health. Participant receives a copy of the plan along with an oral hygiene kit. Participant signs second copy of plan for study records
For any skill, if the interventionist determines the participant has a physical disability and cannot manage the oral hygiene tools, then they may suggest the use of tubing or other options such as foil to adapt the participant’s toothbrush, denture brush or floss holder.



Typodont for Participant Demonstration

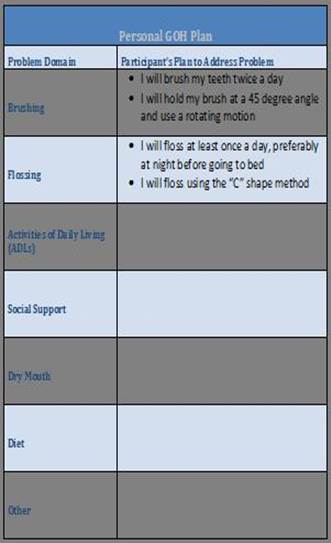
Cognitive Behavioral Plan
Oral Hygiene Kit

Oral Health Campaign
The group-level intervention component of the study, the Oral Health Campaign involves residents as partners in the development of the fairs designed to delivery oral hygiene self-management messages based on the cognitive domains, ADL-related problems in brushing and flossing, brushing and flossing skills, and provide an opportunity to practice brushing and flossing on a mouth model to mastery.
Campaign Committee Training
The oral health campaign begins with the recruitment and training of 5-10 resident volunteers as “oral health ambassadors (or “peer advocates”). A Campaign Committee Consent Form is administered to each prospective Campaign Committee members prior to initiating the Campaign Committee Training. Click here to view the campaign committee consent form. The residents participate in 5-6 weeks of training conducted in English and Spanish and facilitated by the GOH interventionists. During the training residents learn to work together as a team, discuss good oral health knowledge and behaviors, raise and address concerns about promoting good oral health in their buildings, and work with GOH staff to plan and conduct 3 oral health fairs in their buildings.
The volunteer training modules are as follows: Module 1: building group identity and scope of work (committee roles and responsibilities, establishing ground rules and introduction to core theoretical concepts guiding the intervention); Module 2: Review of the components of the Pro-GOH Campaign, protecting and respecting study participants, effective communication; Module 3: oral health and oral health self-management (presentation by collaborating dentist), confirmation of campaign event schedule; Module 4: creation of a campaign plan (selecting messages for each domain 1 – 12); Module 5: development of campaign materials based on module 4; Module 6: preparation for campaign event. Two additional sessions focus on finalizing campaign materials, and practicing testimonials and oral health skills demonstrations and instruction on Practice to Mastery on mouth model. Click here to view the campaign committee training curriculum.
Campaign Preparation and Implementation
Standardized campaign elements of each campaign are created and conducted in English and Spanish and include:
- Campaign messages – based on the study theoretical framework of 12 areas or “domains” that influence a person’s decision to take care of his/her oral health. These domains are:
- Activities of Daily Living (ADLs)
- Oral Health Knowledge
- Oral Health Efficacy – Locus of Control
- Perceived Importance
- Building Level Social Support
- Oral Hygiene Behavior
- Perceived Oral Health Risk
- Self-Management Worries
- Self-Management Fears
- OH Management Intentions
- Dry Mouth
- Diet/Sugar Intake
- Expert mini-lecture plus Q & A – provided by study clinical staff on what is good oral health
- Resident Testimony – shared personal experience on study topic
- Campaign background materials – materials developed in previous GOH projects and by campaign committees
- Campaign recruitment – methods to encouraging residents to attend the oral health fairs including distributing flyers door to door, using posters, and approaching individuals face-to-face.
- Pre-GOH Campaign Activity Guide and checklist – educational games and demonstrations to teach oral hygiene and the importance of take care of one’s mouth. These activities also provide opportunities for correcting misunderstandings, increasing knowledge and addressing barriers to managing one’s oral health.
Click the following to view the manual of procedure
Click the following to view the materials to track participants’ progress during the campaign.